






Key takeaways
• A randomized evaluation of a cash and psychological intervention in Ethiopia shows that offering both elements together in conflict settings improves mental health and economic outcomes.
• Cash improves economic outcomes significantly but has little lasting impact on mental health.
• Conflict weakens intervention effectiveness substantially, reducing gains—especially for mental health.
Republished with permission from VoxDev.
In low-income settings, poverty and mental health are often locked in a vicious cycle. Poor mental health can impair decision-making and reduce productivity, while the stresses of poverty—financial insecurity, food shortages, and environmental hazards—further exacerbate mental illness (Ridley et al 2020). Armed conflict can intensify this cycle: violence and displacement amplify trauma, while the resulting loss of human capital, assets, and jobs pushes households deeper into poverty.
We investigate whether combining psychological support with economic assistance can break this cycle, and how the effectiveness of these interventions shifts in a context of conflict.
The experiment: A multi-pronged approach
Our research was implemented between 2022 and 2024—a period that coincided with the end of the conflict in Northern Ethiopia and a renewed wave of violence in the Amhara region (Hidrobo et al. 2026). We conducted a cluster randomized controlled trial (cRCT) in Amhara and Oromia regions, in which 252 villages were randomly assigned to one of four arms:
- Cash: A one-off lump sum transfer of ETB 15,000 (approximately $279).
- Group therapy (gPM+): A five-session, transdiagnostic group therapy called ‘group Problem Management Plus’, that teaches strategies for stress management, problem-solving, and strengthening social support, and is delivered by non-specialist community health staff.1
- Cash + gPM+: The joint intervention that includes the group therapy and the cash transfer.
- Control: No additional intervention.
Individuals from poor households showing symptoms of mild to moderate depression or functional impairment were invited to join the study. We then tracked 3,055 individuals who enrolled in the study at baseline (before they received any intervention), and again two months later (following the conclusion of gPM+ but before the cash transfer) and 14-18 months later.
Improved economic outcomes but no improvements in mental health
In the 14-18-month follow-up, we find some evidence of enhanced economic outcomes, but limited improvements in participants’ mental health (captured using an index including depression, anxiety, stress, and post-traumatic stress).
Figure 1: Impacts of cash and group therapy on primary outcomes
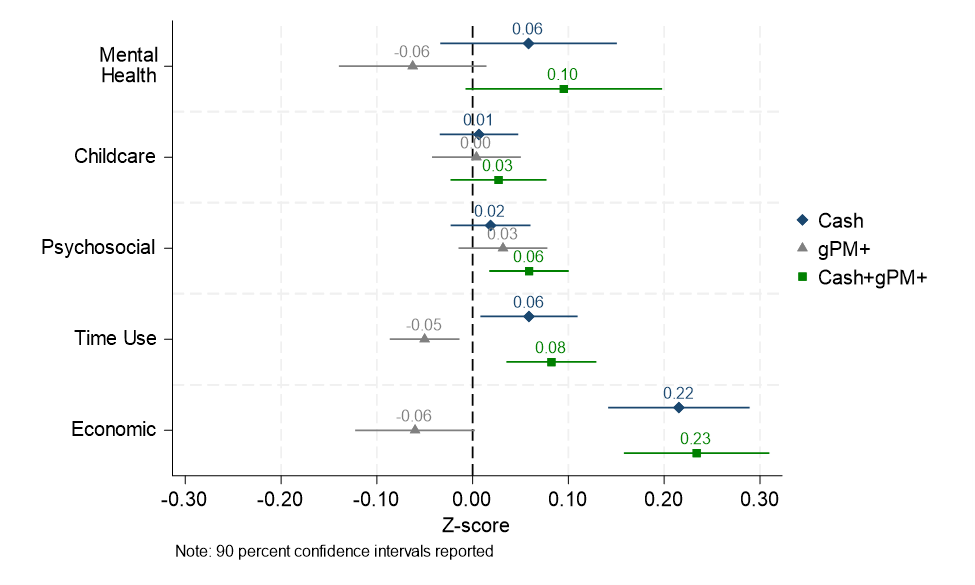
In particular, we find that:
- Therapy alone is insufficient to sustainably improve mental health or economic outcomes. While gPM+ showed some short-term promise, these effects largely faded by the 14-18-month mark. In fact, gPM+ alone had a small negative impact on the time participants spent on income-generating activities.
- Cash drives economic and time-use gains. Recipients of cash saw significant improvements in economic outcomes, particularly in accumulation of assets (like livestock) and savings. They also dedicated more time to income generating activities (such as livestock-related work).
- The “joint” intervention enhances economic outcomes and psychosocial skills, but does not enhance mental health. The combined arm of cash and gPM+ led to the most significant gains in psychosocial skills (such as improved social support and better tension-reduction strategies), income generating time use, and economic outcomes, but had no significant effects on mental health or childcare.
Conflict attenuates improvements in mental health
The positive effects of the interventions were almost entirely concentrated in the Oromia region, where study villages experienced relatively little conflict during the study. In the Amhara region, where intense fighting occurred, we find impacts to be much smaller.
Figure 2: Impacts of cash and group therapy by region
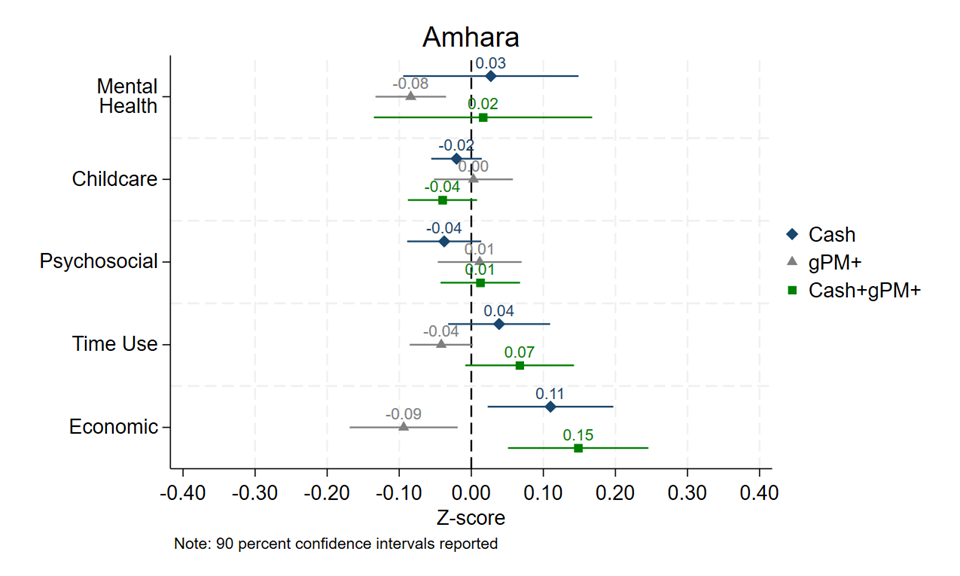
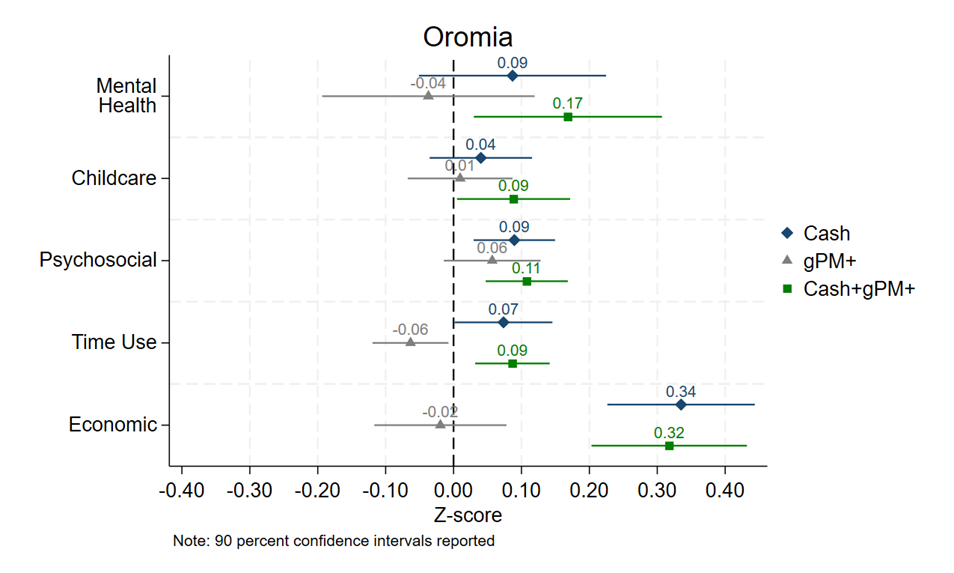
We build on this regional analysis to explore whether a household’s exposure to conflict matters for achieving impacts. Using the Armed Conflict Location and Event Data (ACLED), we find meaningful evidence of variation. In households exposed to zero conflict, the joint intervention leads to enhanced mental health (0.18 standard deviations), psychosocial well-being (0.07 standard deviations), income-generating time-use (0.07 standard deviations), and economic outcomes (0.29 standard deviations). The positive effects of the joint intervention steadily attenuate with increasing exposure to conflict, suggesting that exposure to conflict is a primary reason (though perhaps not the only reason) why the joint intervention did not generally have persistent effects on mental health outcomes in the Amhara region and the pooled sample.
Policy lessons for fragile settings
Our findings suggest that short psychological interventions may not lead to sustained impacts on mental health nor improved livelihoods; however, combining the interventions with cash holds more promise. But even the combined intervention faces challenges in settings with ongoing conflict, either because the acute stress and risk associated with violence makes it challenging to benefit from the interventions, or because any potential short-term gains are destroyed by repeated economic setbacks and trauma.
What does this mean for policymakers?
- Short-term improvements fade: Brief psychological interventions, such as gPM+, can lead to improved mental health in the short term, but impacts may not be sustained over time.
- An integrated approach is the most promising: An approach that simultaneously addresses poverty and mental health is the most promising for sustained improvements in mental health.
- Context is everything: Even interventions that sustainably improve mental health in stable environments may fail in settings with ongoing conflict. In these areas, specialized, symptom-specific interventions targeting severe trauma may be more effective than broad psychological support.
- Cash can still provide benefits in conflict zones: In conflict-affected areas, cash transfers can still provide economic benefits, albeit at a smaller size.
As global conflict reaches record highs, identifying innovative strategies to support affected populations and that effectively deliver services is urgent. Our research highlights that while the path is difficult, the right combination of psychological and economic tools can help individuals begin to reclaim their lives.
Melissa Hidrobo and Jessica Leight are Senior Research Fellows with IFPRI’s Poverty, Gender, and Inclusion (PGI) Unit; Harold Alderman is a Research Fellow Emeritus with IFPRI’s Director General’s Office; Negussie Deyessa is a Professor in the School of Public Health at Addis Ababa University; Daniel Gilligan is Director of PGI; Parthu Kalva is a PhD Student in the Department of Agricultural & Consumer Economics at the University of Illinois Urbana-Champaign; Michael Mulford is Senior Director, Global Poverty Research Lab, Northwestern University; Heleene Tambet is Programs & Data Manager at Enveritas. Opinions are the authors’. This post first appeared on VoxDev.
This work was supported by the U.S. Government and the CGIAR Program on Food Frontiers and Security.
Reference:
Hidrobo, M, H Alderman, N Deyessa, D O Gilligan, P Kalva, J Leight, M Mulford, and H Tambet (2026), “The effects of cash and group therapy in the context of conflict: Evidence from a randomized evaluation in Ethiopia,” Journal of Development Economics, 181: 103724.
1. World Health Organization (WHO) (2019), “Problem management plus (PM+): Individual psychological help for adults impaired by distress in communities exposed to adversity,” Unpublished manuscript.


